
Fat Pad Impingement of the Anterior Knee
Introduction
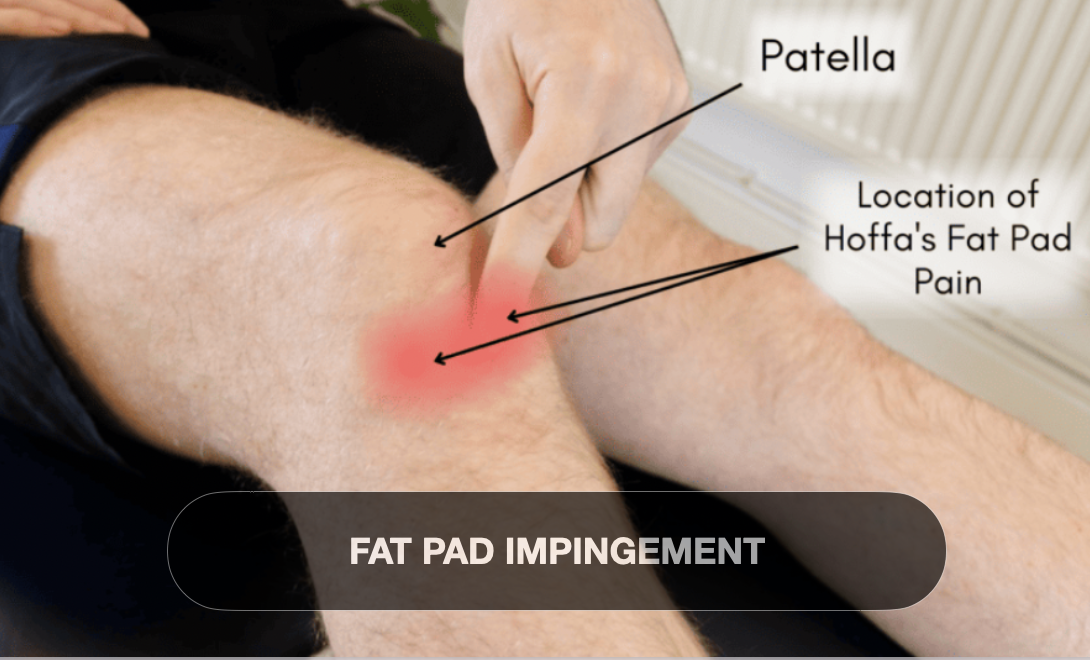
The infrapatellar (Hoffa’s) fat pad is a highly vascularized and innervated soft tissue structure located beneath the patella and behind the patellar tendon. It plays an important role in knee biomechanics, cushioning, and shock absorption. Fat pad impingement—often termed Hoffa’s syndrome—is a frequently underdiagnosed cause of anterior knee pain caused by inflammation and mechanical irritation of the fat pad. Understanding the anatomy, pathomechanics, classification, and clinical presentation of fat pad impingement is essential for physiotherapists to effectively diagnose, treat, and rehabilitate affected patients.
Definition
Fat pad impingement is defined as mechanical irritation and inflammation of the infrapatellar fat pad resulting from repetitive compression or trauma.
The fat pad becomes entrapped between the femoral condyle, tibia, and patella or irritated due to direct injury.
This leads to pain, swelling, and impaired knee function.
It is sometimes called Hoffa’s syndrome or infrapatellar fat pad syndrome and represents a cause of anterior knee pain distinct from patellar tendinopathy or chondromalacia.
Cause
Acute trauma to the anterior knee (direct blow or hyperextension) causing fat pad contusion or hemorrhage.
Repetitive microtrauma from activities involving repeated knee extension and flexion such as running, jumping, and squatting.
Post-surgical changes or altered biomechanics after knee surgery, leading to scarring or increased fat pad impingement risk.
Patellar malalignment or instability resulting in altered fat pad compression.
Overuse syndromes where the fat pad is repeatedly compressed between the patella and femur during knee motion.
Anatomical variants, such as hypertrophy of the fat pad or decreased joint space, may predispose to impingement.
Classification
Fat pad impingement can be categorized based on clinical and imaging findings:
Acute traumatic fat pad impingement: Sudden onset after direct injury or hyperextension.
Chronic impingement: Repetitive overload leading to inflammation, fibrosis, and hypertrophy of the fat pad.
Fibrotic fat pad syndrome: Characterized by fibrotic changes and decreased fat pad elasticity.
Postoperative fat pad syndrome: Occurs secondary to surgical procedures around the knee, such as ACL reconstruction.
Imaging (MRI) can show increased signal intensity in the fat pad, edema, and possible fibrosis, aiding classification.
Signs and Symptoms
Anterior knee pain: Localized just below the patella and behind the patellar tendon; exacerbated by knee extension activities.
Tenderness: Palpation of the infrapatellar region is painful.
Swelling and fullness: May present as a palpable mass or fullness below the patella.
Pain during resisted knee extension or forced hyperextension due to fat pad compression.
Restricted range of motion: Especially in terminal extension because of pain and impingement.
Mechanical symptoms: Some patients report catching or a feeling of tightness anteriorly.
Positive Hoffa’s test: Reproduction of pain with pressure applied to the fat pad during knee extension.
Symptoms may worsen with prolonged standing, stair climbing, or repetitive flexion/extension.
Conclusion
Fat pad impingement of the anterior knee is an important and often overlooked cause of anterior knee pain, primarily due to mechanical irritation of the infrapatellar fat pad. Early recognition through clinical examination and imaging can guide physiotherapists to implement targeted interventions focusing on reducing inflammation, correcting biomechanical faults, and restoring functional movement patterns. Conservative management including activity modification, manual therapy, and specific strengthening exercises often leads to favorable outcomes, while refractory cases may require surgical consultation