
Sinus Tarsi Syndrome
Sinus Tarsi Syndrome
🦶 Introduction
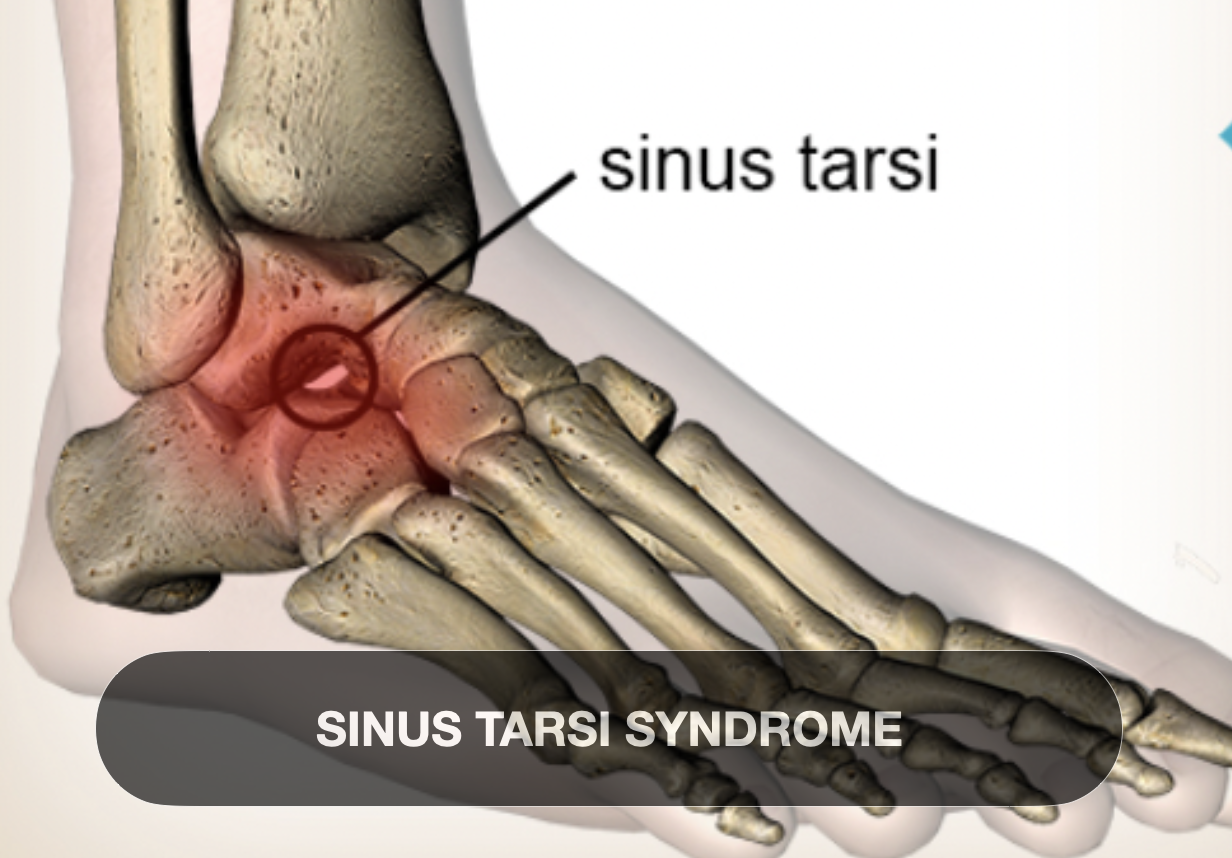
Sinus tarsi syndrome (STS) describes a clinical condition marked by lateral hindfoot pain and a sense of instability, rooted in pathology of the sinus tarsi, a small canal between the talus and calcaneus within the subtalar joint. Although first described by Denis O’Connor in 1957, STS remains a somewhat controversial and multifaceted diagnosis—the term often functioning as an umbrella for various underlying causes such as inflammation, impingement, synovitis, scar tissue, ligament tears, or subtle hindfoot instability
✅ Scientific Summary
1. Definition
A syndrome marked by pain and tenderness localized to the sinus tarsi region, often accompanied by a sensation of subtalar instability
Broadly descriptive rather than a precise pathological entity; synonyms include "sinus tarsi pain," "sinus tarsi impingement," and “tarsal sinus syndrome”
2. Cause
Primary: Acute or recurrent inversion ankle sprains (~70–80% of cases) leading to injury of subtalar ligaments (interosseous talocalcaneal, cervical, etc.) and subsequent synovitis, hemorrhage, fibrosis, or scar tissue in the sinus tarsi Secondary: Biomechanical factors such as overpronation, flatfoot deformity, excessive joint eversion/inversion, or chronic subtalar instability (~20–30%) Less often linked to degenerative joint disease, ganglion cysts, or inflammatory arthritides (e.g., rheumatoid arthritis)
3. Classification
No formal staging system exists; STS is best described as symptomatic sinus tarsi pain with or without mechanical instability
A “canalis tarsi syndrome” variant may present with broader, medial hindfoot symptoms
Suggested best practice is to identify underlying causes (e.g. ligament tear, impingement, synovitis) rather than rely on the general label
4. Signs & Symptoms
Pain: Deep, lateral hindfoot ache or sharp stabbing at the sinus tarsi; exacerbated by palpation, inversion/eversion, weight-bearing, walking uneven terrain
Tenderness to direct palpation over the sinus tarsi, reproducible with supination and adduction
Instability: Reports of looseness, giving-way, especially with uneven surfaces or direction changes
Associated findings: Subtalar range-of-motion restriction, potential peroneal spasms, valgus hindfoot posture in some cases
Diagnostic injection: Pain resolution with local anaesthetic in the sinus tarsi is considered confirmatory
5. Current Treatment Trends
A. Conservative First-line (~60–80% success)
Rest/immobilisation (e.g., ankle braces, crutches) to reduce irritation
NSAIDs, cryotherapy, activity modification
Physical therapy: Targeted proprioceptive and neuromuscular training, strengthening of calf, foot and ankle, joint mobilisations, balance/coordination drills, retraining motion patterns
Supportive devices: Footwear modifications, off-the-shelf or custom orthoses, medial heel wedges
Injections: Local corticosteroid/anaesthetic, platelet-rich plasma or ozone injections into the sinus tarsi space — effective for short-term relief
B. Minimally Invasive / Interventional (~40–60% success)
Ultrasound- or fluoroscopy-guided injections of corticosteroid or biologicsSubtalar arthroscopy: Diagnostic and therapeutic debridement of synovitis, scar tissue, ligament repair — increasingly favored when imaging is inconclusive and conservative measures fail
C. Surgical Intervention (rare; for refractory cases)
Open or arthroscopic debridement, removal of bony or soft-tissue impingement, ligament reconstruction, or in structural deformities, procedures such as subtalar arthroereisis for flatfoot correction
Post-surgical rehab includes immobilization followed by progressive rehbilitation therapy, aiming for return to sport or full function in 4–6 months; full recovery by ~12 months 6. Prognosis
Excellent outcomes with early, comprehensive conservative care; persistent symptoms risk chronic instability and pain
Minor relapse rates exist if only conservative methods are used.
Arthroscopy offers ~60–70% return-to-sport success; provides both diagnostic clarity and therapeutic effect